
White Plague, Black Death: Public Health as a Weapon in South Africa and the USSR
Nineteenth century European Romantic writers viewed tuberculosis as a fashionable disease. The slow but inexorable progression of the “white plague” (or consumption) and the austerity of the pale, emaciated (white) bodies of those suffering from it gave rise to pathos-infused works by Keats, Verdi, Dostoyevsky, and other notable writers, painters and composers.

In the twentieth century, with a much greater concern for communist orthodoxy than aesthetics, the Soviet government made tuberculosis inevitable for its citizens, particularly those like Aleksandr Solzhenitsyn who served time in forced-labor camps. Similarly, in apartheid-era South Africa tuberculosis disproportionately afflicted disenfranchised blacks more than privileged whites. Government officials there also profited politically and financially off blacks relegated to work camps for the mentally ill.
Public health has not always been pursued in the public interest; sometimes it’s been used by elites as a tool for political repression and financial gain. Readex’s unique collection, Public Health: Global Origins of Modern Health Policy and Management, 1957-1995, brings to light both the benefits and deficiencies of public health policy during the latter half of the twentieth century.
Drawn from Readex’s comprehensive Joint Publications Research Service (JPRS) Reports, 1957-1995, the new Public Health collection retains that database’s focus on communist and authoritarian countries. One of the most compelling features of the Public Health collection is that it covers nearly the entire span of both the Cold War and institutionalized apartheid.
With regard to the former, it allows us to get beyond the checkpoints and barbed wire of the Gulag (Soviet forced-labor camps) to learn the public health consequences of systematic oppression and political dysfunction. As we will see, it even gives us a glimpse into the mind of Josef Stalin himself.
Epidemic Tuberculosis in the Soviet Union: The Gulag Connection
The Gulag [Glavnoye Upravlenie Lagerei, “Main Administration of Camps”] system of forced-labor camps received exiled petty criminals, political dissidents and numerous other undesired ethnic and economic classes of persons to harsh conditions in remote regions of the Soviet Union. The Gulag lasted nearly as long as the USSR itself, although its use was most prevalent during the rule of Josef Stalin from about 1930 until his death in 1953. Over 15 million people were imprisoned in these camps, often on spurious charges. Many internees died there. Unsurprisingly, public health was an afterthought—except when it was intentionally subverted.
O. Chegodayeva, writing in Komsomolskaya Pravda [Komsomol Truth] in 1990, described how little the contributing factors of tuberculosis had changed since the time of Anton Chekhov, the famous author and physician (who himself suffered from tuberculosis):
“The harsh climate, all sorts of deprivations suffered in the work, in escape attempts and in confinement, the turbulent life in common wards, the lack of fat in the food, yearning for home—these are the main causes of consumption on Sakhalin.” was the conclusion drawn by Dr. A. Chekhov following a visit to the “convict island” of Sakhalin in 1890, which was a Prussian prison at that time. Here is a statement from a contemporary study: “the psychological and emotional stress caused by being arrested, isolation from society, replacement of the accustomed way of life, the food ration, unsatisfactory communal living conditions (particularly in the wards), and heavy labor negatively affect the defensive forces of the convicts.” These two quotes are 100 years apart, but the fatality list has not changed at all.

Valeriy Abramkin, writing in Moskovskiy Komsomolets [Moscow Komsomol] in 1992, took Chekhov’s and Chegodayeva’s critiques a step further:
The high incidence of tuberculosis is the result of purposeful actions by prison and camp personnel, and of existing penitentiary policy and practice directed at destroying certain groups of criminals and prisoners.
When buildings are erected in many prisons and camps for the punishment of “violators” (punishment cells, penal isolation cells, PKT [not further identified]), special steps are taken to create elevated humidity, poor ventilation, low temperature in winter and high temperature in summer in these spaces. For example salt or other chemicals are mixed into concrete and slurry during construction, the floor is laid beneath ground level, the first waterproofing layer (roofing material) is laid at ceiling level, poor heating systems are installed, windows are blocked with sheet iron, and so on. Patients with the active form of tuberculosis are placed in the same cells with healthy inmates in spring and fall. At the direction of workers of the operations section, doctors who reveal disease in an inmate do not report it to him, they do not prescribe treatment to him, and they do not send him to the hospital.
All this means that Russian camps are camps for the destruction of people, and the GULAG is working essentially at undermining the health of the entire nation, and setting the stage for the spread of the tuberculosis epidemic outside the prisons into the public at large.
Citing an estimate by Natalya Vezhnina, chief physician of Russia’s largest tuberculosis clinic, Abramkin states that:
…the incidence of tuberculosis in the GULAG is 35 times higher than outside it, the cure rate is only 20-30 percent for this disease, while for the most severe forms it is only 3 percent.
Such that it can be stated with full certainty that a tuberculosis epidemic is raging in our prisons and camps. Moreover in Vezhnina’s opinion this epidemic could spill over into the public at any time. The fact is that only 7-10 percent of tuberculosis patients released from confinement are put on record in antituberculosis dispensaries and continue with their treatment; the rest become carriers of the disease, and unlike what is true for AIDS, you can’t save yourself from tuberculosis with a condom (tuberculosis is readily transmitted by aerosol).
Chegodayeva gives a more insidious reason why tuberculosis could run rampant in the general population: it was advantageous to have it. She refers to the Romantic view of the disease and then adds a sinister caveat:
Tuberculosis is also described as the “royal disease.” Victims of tuberculosis frequently do not suffer any outward symptoms. A person with considerable damage to the lunges [sic] may feel perfectly tolerable. The hospital gates are open, and it is not forbidden to take walks in the fresh air. What a life! No need to work, one feels fine and is fed to the tune of 1 ruble and 70 kopecks a day; he can come and go as he pleases; the hospital allowance is paid on a regular basis.…One can drink. He will not be discharged; he could infect others.
But there is yet another reason—the main one, in my view—why the patients are in no hurry to get well. It is profitable to have tuberculosis in our society. It is the only chance many people have to escape the difficult social circumstances in which they find themselves. For prisoners it means trading a bunk for a hospital bed, performing lighter work and receiving better chow. For others it means escaping from communal apartments and dormitories. The Council of Ministers has issued a special decree granting the right to housing out of turn for tuberculars. But this is only for the infectious patients. If they get well, they lose their benefits.
Lest the true nature and purpose of Soviet labor camps be confused with economic redemption for either the prisoners or the nation, in his monograph On Stalin and Stalinism: Historical Essays Roy Medvedev recalls a chilling feature of the Kolyma labor camp in the Soviet Far East.
Incidentally, over the entrance to all camp center divisions of Kolyma hung the motto prescribed by the camp statute: “Labor is a matter of honor, valor and heroism.” We remember the inscription on the gates of Auschwitz: “Work makes free” [Arbeit macht frei].
So how did this pernicious system sustain its hold on a people who had overthrown the tsar for similar injustices? During President Mikhail Gorbachev’s Glasnost [openness] and Perestroika [restructuring] campaigns in the mid-1980s prior to the dissolution of the Soviet Union in 1991, journalists and historians gained unprecedented access to archival material and a relatively uncensored press. Readex’s Public Health collection includes content from those crucial few years when the former Soviet citizens were sifting through the ruins of their empire, before the elites reconsolidated their power.
In 1988 psychiatrist Mikhail Buyanov gave some thought to Stalin’s mental health in an article entitled, “A Sick Society, or a Sick Leader?” He noted Stalin’s fear and persecution of doctors, and the “doctor’s plot” from 1951-53 when Jewish physicians were accused of planning to assassinate Soviet leaders. Doctors were arrested and tortured, and were only spared when Stalin died in March 1953.
While asserting that Stalin was to a great extent a product of turbulent times and did not manifest obvious schizophrenic or delirious behavior, Buyanov does not hesitate to classify Stalin as a psychopath.
The hero of our essay can be categorized within this group of borderline patients, specifically, to the psychopath group. Stalin’s personality was grave—he was gloomy, suspicious, ruthless and egoistic. I would place Stalin among those unique personalities which, in their most phenomenal form, have concentrated within themselves everything characteristic of tyrants, sick and healthy alike. Stalin can be considered a paranoiac and psychopath with tendencies towards delirium but, just as the key must fit the door for it to open, so the nature of a personality must correspond with the environment to create a tyrant. Without an appropriate environment, Stalin would be just a petty egoist, a waning personality full of envy and obsessed with a passion for considering himself greater and more intelligent than others.
Stalin is no maniac in the medical sense. He is a maniac in the social meaning of the word. An insatiable thirst for power, hypocrisy, unquenched ambition, incinerating treachery, cold hatred towards everybody who doubted him as the chosen one, detached and thoroughly pondered political calculations devoid of moral limitations, of any emotion, of any artistic improvisation—this was Stalin.
Buyanov was not the first physician to warn the public of the disastrous consequences of having a psychopath as chief executive. There was also Russian neurologist Vladimir Bekhterev. Stalin had likely coopted physicians to end Vladimir Lenin’s life so he knew that they could threaten his own grip on power. For that reason he had Bekhterev poisoned in 1927 when he learned that in Bekhterev’s professional opinion he was a psychopath.
The assassinated doctor’s wife disappeared soon after his death. Most of his relatives ended up in the Gulag. His work was effaced from textbooks. Buyanov cites other instances of physicians coming to bad ends when they spoke truth to power. It was much easier and safer for professionals at every level to indulge the whims of dictators. One can argue that this is still the case.
Illusory Mental Illness, Conspicuous Consumption (for Blacks): South Africa
South Africa had its own take on mental illness; apparently black South Africans suffered from it much more frequently than did whites, and with more dire results requiring more sustained courses of treatment. This was actually true for tuberculosis, but first a story related by Belgian journalist Paul Emmanuel in 1977 in his article, “The Last Slaves.” Emmanuel describes the discovery of a covert sanatorium devoted to ends inimical to mental health.
On 9 August 1970 a white traveler lost on the plains saw a group of barracks in the distance. He went there to ask the way to Johannesburg, and discovered the hallucinatory universe of the West Rand Sanatorium—from 20 to 200 “patients” to a room, depending on the size of the room, living on the bare ground or on pallets covered with matting that each one had to make for himself, since the establishment hardly furnished any… Patients who, for want of care, soil what serves them as a bed, and whom their jailers, concerned about hygiene, sluice down each morning with a fire hose. By way of nourishment, soy beans, a few potatoes, from time to time a meat ball, unsweetened tea and coffee for breakfast, served in buckets to which human beings in the condition of animals come to dip out their portions in empty tin cans… As for the “therapeutic occupations,” which these living dead do not practice for the simple reason that they are subjected to them, they consist of working 10 hours a day in the fields, printing baggage checks for various airlines, making belts or clothes brushes…
The errant traveler was a sincere Christian whose church had a relationship with Amnesty International, so he informed the local and international press. After considerable government stonewalling it came to light in 1974 through Per Wästberg, a Swedish journalist, that the West Rand camp and others like it were places where blacks hastily diagnosed as mentally ill were sent as slave labor for international conglomerates.
While there, they were subjected to unspeakable living conditions, were routinely sedated, given electroshock treatment without anesthesia, and in some cases prefrontal lobotomies. The World Health Organization (WHO) was damning it its report:
“In the Republic of South Africa,” this preliminary study states, “between 8,000 and 9,000 Africans suffering from mental disorders are confined against their will in private establishments. They are the subject of a deal between the state and certain commercial enterprises belonging to whites which ensure the custody of mental patients designated in a government publication as ‘the dregs of the mental misfits and deviants.’ These commercial enterprises receive a subsidy from the government for each patient interned. There is not a single black psychiatrist in South Africa, and vital decisions concerning thousands of African mental patients are made by part-time doctors who do not even speak their language.
This is the opposite of public health; the author describes the situation as reminiscent of Solzhenitsyn’s Gulag Archipelago and Nazi death camps. And it gets worse:
These barbarous practices and this scientific degradation of the “patients” are justified, if we may use the term, by the fact that the great majority of those interned are perfectly well-balanced individuals. In reality the providers of these “sanatoriums” are not physicians but policemen, those of the Newlands commissariat at Johannesburg especially, who are permitted by law to consider blacks who are drunken or intractable as “antisocial” and have them locked up without any other form of trial.
In response to international outrage conditions improved somewhat. The official denials continued but the walls of the facilities were whitewashed, blue curtains were hung in the windows. Blankets were provided (in the summer). And the profits continued to roll in. Like the Soviet and Nazi camps, the sanatoria were administered systematically under the rubric of social and economic development.
There are 13 private “sanatoriums” in South Africa, including Randfontein with its 5,090 patients, Poloko, whose inmates revolted 2 years ago, Simmer and Tabamoopo, Allanridge, Ekuhlengeni-Kwamakuta, East Rand, and West Rand… All belong to the firm of Smith & Mitchell, controlled by the multimillionnaire [sic] David Tabatznik, of Polish origin. The latter was formerly the right hand man of a certain Richard Lawrey (or Lurie), president of the board of directors of the investment firm Protea, of which Smith & Mitchell is one of numerous subsidiaries.
Through Smith & Mitchell, Tabatznik has a monopoly on the construction and equipping of ultramodern hospitals reserved for whites, such as the famous Groote Schuur at Capetown, where Prof. Barnard operates, and Protea, in turn, is the most important stockholder of the Standard Bank of South Africa, which controls practically the whole of the pharmaceutical production and distribution.
But Standard Bank itself is controlled by Chase Manhattan Bank of New York, and to say Chase is to say Rockefeller; i.e., immense interests in South Africa…
Not all the Gulags are in Siberia, and apartheid is not exclusively South African.
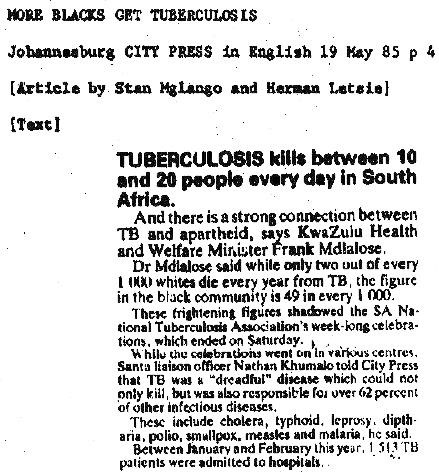
In the Soviet Union or in South Africa, a return to the Gulag means a return to tuberculosis. How fared that malady in South Africa? According to journalists Stan Mglango and Herman Letsie, tuberculosis in South Africa was enjoying brilliant success in 1985, but only among the black population. For whites it was still fairly rare:
Tuberculosis kills between 10 and 20 people every day in South Africa.
And there is a strong connection between TB and apartheid, says KwaZulu Health and Welfare Minister Frank Mdlalose.
Dr. Mdalose said while only two out of every 1000 whites die every year from TB, the figure in the black community is 49 in every 1000.
These figures shadowed the SA National Tuberculosis Association’s week-long celebration, which ended on Saturday.
While the celebrations went on in various centres, Santa liaison officer Nathan Khumalo told City Press that TB was a “dreadful” disease which could not only kill, but was also responsible for over 62 percent of other infectious diseases.
These include cholera, typhoid, leprosy, diphtheria, polio, smallpox, measles and malaria, he said.
Between January and February this year, 1513 TB patients were admitted to hospitals.
And so we come full circle. As with disease, there is a natural cycle to political and economic oppression. Public health at times promotes private interests at the expense of the commonweal.
With the COVID-19 pandemic restructuring global relationships literally at the cellular level, the historical record as captured in Readex’s Public Health: Global Origins of Modern Health Policy and Management, 1957-1995, can offer valuable guideposts to help inform policy and practice. Unfortunately—and fortunately—we have been here before. In responding to despotism and racism as to epidemics, there are lessons to be learned from the past.


